

Introduction
Von Willebrand factor (VWF) multimer analysis is an essential tool in the diagnosis and classification of von Willebrand disease (VWD). Current visual VWF multimer analysis is observer dependent, time consuming and is inaccurate in detecting subtle changes in multimer patterns. Therefore, recent studies have investigated VWF multimer quantification using semiautomatic densitometric analysis. The accuracy of VWF multimer densitometric analysis in clinical practice needs further investigation before it can be widely used. The aim of the study was to validate the accuracy of VWF multimer densitometric analysis in clinical practice. Additionally, we aimed to identify patient characteristics associated with VWF multimer densitometry outcomes in type 1 and type 2 VWD patients, and we investigated whether subtle differences in VWF multimer pattern are associated with the bleeding phenotype of VWD patients.
Methods
We included patients from the nationwide Willebrand in the Netherlands (WiN) study. The inclusion criteria of the WiN study were a personal hemorrhagic diathesis or family history of VWD, and historically lowest VWF antigen (VWF:Ag), VWF activity (measured with the monoclonal antibody assay: VWF:Ab) or VWF collagen binding (VWF:CB) ≤0.30 IU/mL or FVIII activity (FVIII:C) ≤0.40 IU/mL in case of type 2N VWD. At inclusion in the WiN study, blood was drawn and patients filled in an extensive questionnaire containing a self-administered Tosetto bleeding score (BS).
For multimer analysis, citrated blood samples were separated on 0.9% agarose gel and visualized by Western blotting. We used IMAGEJ for densitometric analysis. The five smallest bands on densitometric images were defined as small multimers, next five bands were defined as medium multimers and the remaining bands were defined as large multimers. Medium-large VWF multimer index was calculated by dividing the patient's multimer ratio (intensity of the medium and large multimers divided by the total intensity of all multimers) by the multimer ratio of a normal control in the same western blot. If no multimers could be detected, the multimer index was set as 0.
Results
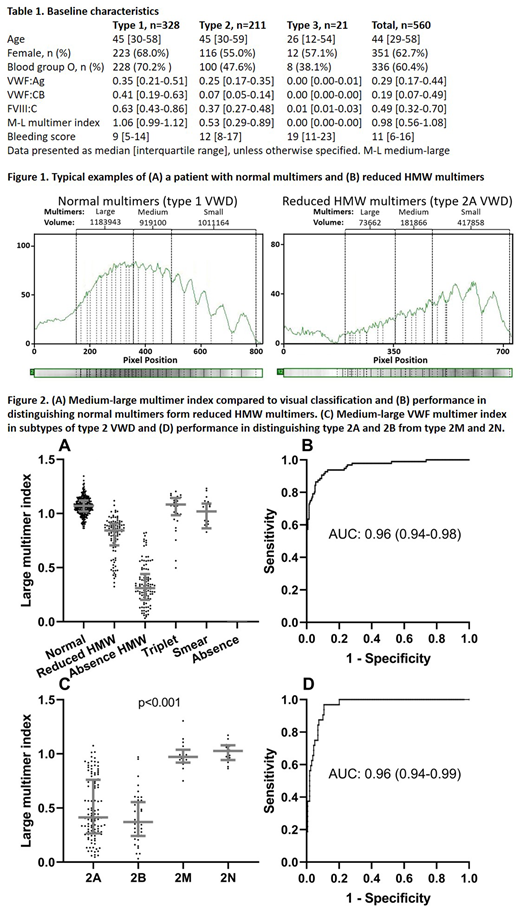
We included 561 VWD patients: 328 type 1, 211 type 2 and 21 type 3 patients. The median age was 44 [IQR 29-58] and 351 patients (62.7%) were female (Table 1). Figure 1 illustrates typical densitometric outcomes of a type 1 VWD patient with normal VWF multimers (A) and a type 2A patient with reduced high-molecular-weight (HMW) VWF multimers (B).
Medium-large VWF multimer index was 1.06 [0.99-1.12] in type 1 and 0.53 [0.29-0.89] in type 2 and 0.00 [0.00-0.00] in type 3 VWD. Medium-large VWF multimer index was in patients visually classified as normal, reduced and absent HMW VWF multimers, respectively 1.07 [1.02-1.12], 0.84 [0.71-0.91] and 0.31 [0.20-0.44] (p<0.001, Figure 2A). With visual examination as gold standard, medium-large VWF multimer index had a very good accuracy in distinguishing normal VWF multimers from reduced HMW VWF multimers (AUC: 0.96 (0.94-0.98) p<0.001, Figure 2B). It could also accurately distinguish reduced HMW VWF multimers from absence of HMW multimers, with an AUC of 0.95 (0.92-0.97, p<0.001), and type 2A and 2B from type 2M and 2N (AUC: 0.96 (0.94-0.99), p<0.001, Figure 2C and 2D).
From VWF activity measurements, medium-large VWF multimer index was strongest correlated with VWF:CB (ρ=0.79, p<0.001). From the ratio of the various functional VWF measurements (divided by VWF:Ag), the strongest correlation was again found for VWF:CB/VWF:Ag ratio (ρ=0.80, p<0.001).
In type 1 VWD, an increased clearance of VWF (defined as VWFpropeptide/VWF:Ag ratio ≥2.2) was independently associated with lower medium-large VWF multimer index (β=-0.10 (-0.14; -0.07), p<0.001). Also, type 1 VWD patients with a VWF gene variant had relatively lower medium-large VWF multimer index compared to type 1 patients without a VWF variant, respectively 1.03 [0.95-1.10] vs 1.08 [1.04-1.12] (p<0.001).
In the total population, higher medium-large VWF multimer index was associated with a lower bleeding score: β=-4.6 (-7.2; -2.0), p=0.001, adjusted for age, sex, blood group and type of VWD.
Conclusion
Semiautomatic densitometric analysis of VWF multimers has an excellent accuracy in clinical practice, and may have an additional value in providing a better understanding of the clinical features such as the bleeding phenotype of VWD patients.
Atiq:CSL Behring: Research Funding; SOBI: Other: travel grant. Boender:SOBI: Current Employment; CSL Behring: Research Funding. Cnossen:Bayer: Research Funding; Novo Nordisk: Research Funding; Nordic Pharma: Research Funding; Sobi: Research Funding; Takeda: Research Funding; CSL behring: Research Funding; Pfizer: Research Funding; Shire: Research Funding; Baxter: Research Funding. van der Bom:Bayer: Speakers Bureau. Fijnvandraat:SOBI: Research Funding; NovoNordisk: Consultancy; Grifols: Consultancy; Takeda: Consultancy; Roche: Consultancy; CSL Behring: Research Funding; NovoNordisk: Research Funding. Van Galen:Bayer: Research Funding; Takeda: Speakers Bureau; CSL Behring: Research Funding. Laros-Van Gorkom:Baxter: Other: Educational grant; CSL Behring: Other: Educational grant. Meijer:Bayer: Research Funding; Sanquin: Research Funding; Pfizer: Research Funding; Bayer: Speakers Bureau; Sanquin: Speakers Bureau; Boehringer Ingelheim: Speakers Bureau; BMS: Speakers Bureau; Aspen: Speakers Bureau; Uniqure: Consultancy. Eikenboom:CSL Behring: Research Funding; Roche: Other: Teacher on educational activities. Leebeek:Roche: Other: DSMB member for a study; SOBI: Other: Travel grant; Novo Nordisk: Consultancy; Shire/Takeda: Consultancy; Uniqure: Consultancy; Shire/Takeda: Research Funding; CSL Behring: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal